Before presenting the details of the topic, it is worth noting Young Lee’s qualifications: he is a licensed acupuncturist in the States of NJ and NY. He is a Diplomat in Acupuncture certified by the NCCAOM. He holds an MS degree from Tri-State College of Acupuncture, the acupuncture school that taught ‘trigger point needling’ using the textbook by Simons and Travell ‘The Trigger Point Manual”. He holds several patents on needling devices (US Patent 5735868,1996; US Patent 5996167, 1999; US Patent 6117155, 2000; US Patent 2021/0378911, 2021).

Symptoms that can be treated with trigger point needling in the upper body include tension headache, neck pain, shoulder pain, arm pain, tennis elbow, golfer’s elbow, wrist pain, and numbness and tingling in the fingers.
Symptoms that can be treated with trigger point needling in the lower body include sciatica, low back pain, hip pain, thigh pain, knee pain, hamstring pain, foot pain, and numbness and tingling in the toes.
There have been several major developments in trigger point needling. In 1973, Gunn introduced intramuscular stimulation – a dry needling method – for treating chronic pain. In 1983, Simons and Travell published “Trigger Point Manual,” which introduced a detailed description of trigger points. In 1994, Hong presented clinical data showing that dry needling with a local twitch response is the most effective for treating pain symptoms. In 2003, Shah and others at the National Institutes of Health experimentally confirmed that pain chemicals disappear after an LTR elicitation.
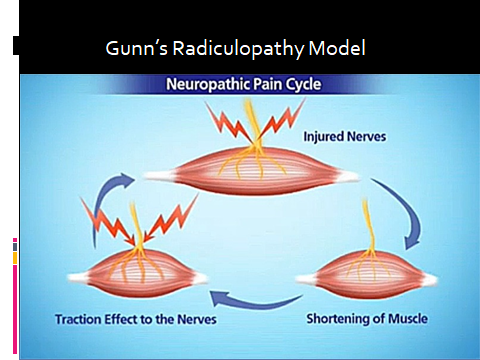
Gunn postulated that chronic pain is due to nerve injury at the level of the nerve root during an accident, which results in muscle shortening. This shortened muscle pulls on the muscle, further shortening the muscle fibers. This traction effect further injures the nerve root, and the effect is sustained in a vicious cycle. This is called the Gunn’s radiculopathy model for chronic pain.
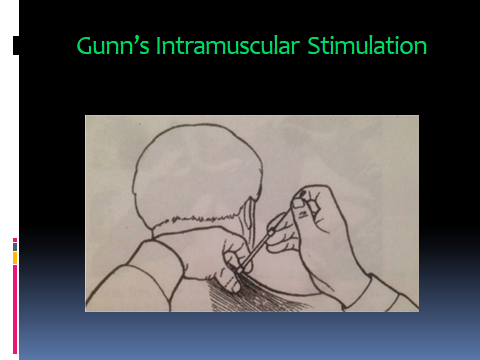
Gunn treated chronic pain by inserting a needle into the region of muscle shortening. The needle is left in place for some time (just as in traditional acupuncture), or it is moved up and down (this is called ‘dry needling’) to stimulate the shortened muscle and relax the shortening. He did not mention local twitch response (LTR) specifically.
Simons and Travell wrote two books on ‘Myofascial Pain and Dysfunction’ for Upper and Lower Extremities, respectably, as shown here. These books were used as textbooks in my former acupuncture school, Tri-State College of Acupuncture, headed by Mark Sim. These two books were used to train students on trigger point needling, along with traditional acupuncture. Mark Sim called the trigger point needling Acupuncture Physical Medicine.
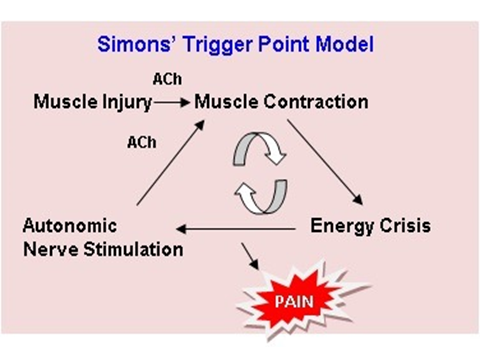
Simons proposed a different view of the vicious pain cycle based on muscle injury. When a muscle is injured, acetylcholine is released, and this causes muscle contraction. Increased energy demand in this contraction zone results in an ischemic condition. This creates an energy crisis there. This, in turn, stimulates the autonomic nervous system, which releases acetylcholine and pain chemicals. The acetylcholine causes further muscle contraction, thereby maintaining the vicious pain cycle. The pain chemicals released cause pain.
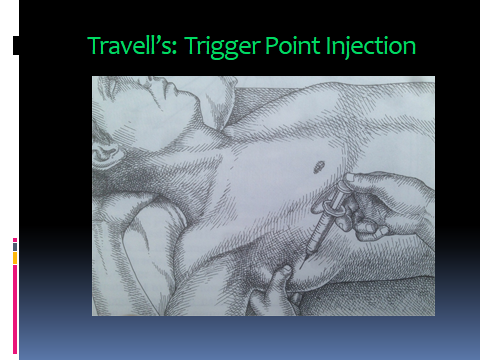
Trigger point injection used by medical doctors to reduce pain is suggested by Travell. The medications injected include lidocaine (for short-term pain relief), corticosteroids (to reduce inflammation), or saline. When no medication is injected, it is called ”dry needling”. Hong found that dry needling alone is often more effective than ‘wet’ needling of injecting medications.
Dr. Hong of University of California Irvine discovered that eliciting Local Twitch Responses during dry needling is essential for maximum effectiveness of pain relief.
In my opinion, this is the most significant finding in the field of pain management.
Hong discovered that if a needle is placed in an area of contracted muscle fibers, the muscle would twitch spontaneously (Hong, 1994). He observed that this local twitch response (LTR) breaks the shortening of muscle fibers and relaxes the muscles. This allows the muscle to fully relax, breaking the pain cycle and enabling healing.
The LTR does three things: it relaxes the muscle to restore the original tension; it breaks the vicious pain cycle; and it prevents muscle contraction.
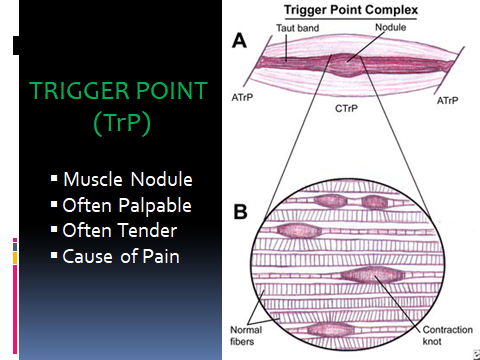
The trigger point region consists of muscle knots from muscle-nerve interaction stemming from injury. Muscle knots form a muscle nodule, which is often palpable and tender when pressed. When a muscle has a lot of contracted fibers, the whole muscle becomes shortened and this results in compression of blood vessels and nerve branches in the trigger point region. This causes compression pain in the involved muscle. Sometimes, the range of motion becomes limited. The shortened muscles also pull the muscles that are attached to the bone. This creates ‘pulling’ pain at the level of joint, as in ‘tennis elbow’.
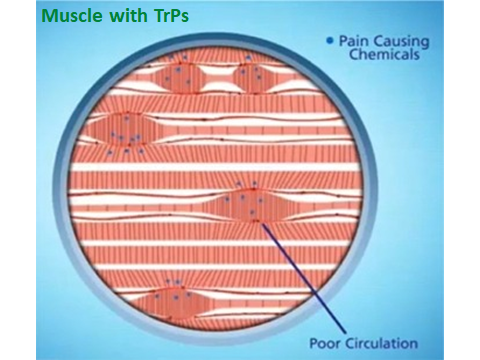
Shah and his collaborators at NIH collected a fluid sample from a trigger point before and after LTR, respectively. From the sample before eliciting a LTR, they were able to detect pain-causing chemicals.
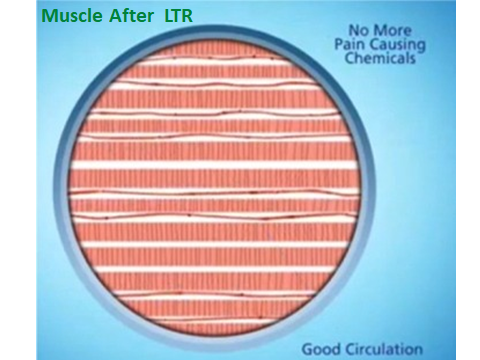
But from the sample collected at the same point after eliciting a LTR, pain chemicals were not detected. This is an experimental proof of Hong’s finding that pain is eliminated after eliciting a LTR.

At Tenafly Acupuncture, we palpate injured muscles to find trigger points. These points are then needled with acupuncture needles to elicit local twitch responses (LTRs).
When a patient experiences pain due to an injury, there are many trigger points in the involved muscles.
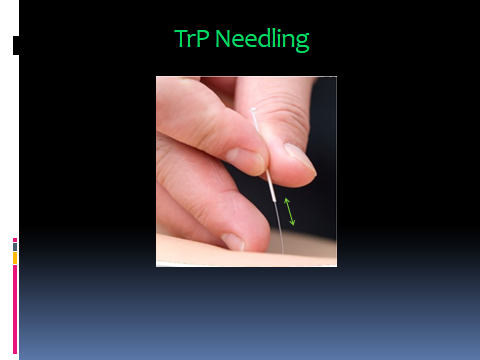
An acupuncture needle is inserted into a tight trigger point in the ropy muscle band, and the needle is moved up and down to elicit local twitch responses (LTRs).
LTRs elicited are classified in terms of their twitching strength: patient-feels-only LTR (referred to as ‘EMG level in the picture); LTRs that are palpable by fingers of the practitioner; LTRs that are visible to the practitioner; and forceful LTRs that involve the contraction of the entire muscle band.
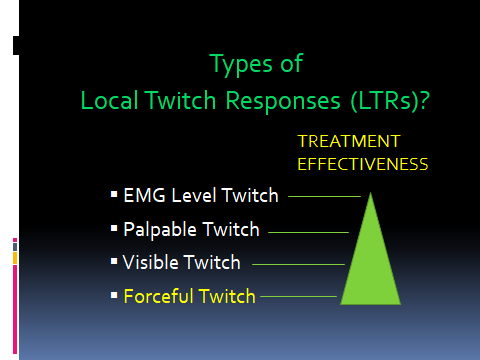
Pain relief is proportional to the strength of the LTR – forceful twitches are the most effective.